Tension-Type and Cervicogenic Headache
Posted by Phil Heler, MD on December 20, 2019The most common headaches are tension-type headache and cervicogenic headache.
Statistically the most common types of headaches irrespective of causative factors are tension-type headache (up to 40-50% in some populations) and cervicogenic headache (20-30%).

The last two pieces I have written have discussed stress and then its association with migraine. However, the incidence rate for migraine is of course much lower than other forms of headache.
The earliest Ancient references to headaches can be found in the Ebers Papyrus which were purchased in 1872 by the Egyptologist George Ebers, for whom the papyrus is named. One passage dates the papyrus to the 9th year of the reign of Amenhotep the First which would place the papyrus to around 1534 BC. This is a compilation of oldest known medical texts. The scroll contains 700 magical formulas and folk remedies meant to cure afflictions ranging from crocodile bite (handy in Derbyshire!) to toenail pain and headaches. This is not surprising as headache disorders are among the most common disorders of the nervous system.
The Main Types of Headache: Primary vs Secondary
The International Headache Society has identified 13 broad categories of headaches and 128 distinct disorders which vary in their commonality!
Headache itself is a painful and disabling feature of a small number of very common primary headache disorders, namely migraine, tension-type headache, and cluster headache. Headache can also be secondary to a long list of other conditions, the most common of which we see in clinic setting is a cervicogenic headache (or pain from anatomical structures in the neck); although in general medication-overuse is the most common.
There is a large cost to society when it comes to headaches of any kind, most of these are indirect such as time spent off work. On the individual level, headaches cause disability, suffering, and loss of quality of life that is on a par with other chronic disorders.
On a broader scale it may sound strange but there is an association between lower back pain and headaches. A recent study published in the Journal of Headache and Pain this year discovered a correlation between these very two different types of pain. The researchers from Warwick Medical School were funded by the National Institute for Health Research (NIHR) to undertake a systematic review of fourteen studies of which 195 participants attempted to quantify the association between persistent headaches and lower back pain. Their conclusions revealed an unexpected correlation between the two. Around 1 in 5 people have persistent low back pain and 1 in 30 have chronic headaches; although the type of headache was not specified. The researchers estimate that just over 1 in 100 people (or well over half a million people) in the UK have both. Professor Martin Underwood, from Warwick Medical School, said: “In most of the studies we found that the odds were about double — either way, you’re about twice as likely to have headaches or chronic low back pain in the presence of the other. Which is very interesting because typically these have been looked as separate disorders and then managed by different people. But this makes you think that there might be, at least for some people, some commonality in what is causing the problem.”
Tension-Type Headache
The two main types of headaches we see are usually tension-type headache (or TTH) and cervicogenic headaches which are often related directly or indirectly with an accompanying musculoskeletal complaint.
Tension-type headaches are termed as primary headaches as they are not the result of another medical condition. A TTH usually causes pain on both sides of the head with mild-to-moderate intensity. The pain is often described as a pressing or dull ache, lasting between 30 mins or, at worst, even up to a week.
Headaches these days even have their own classification system. The International Classification of Headache Disorders (ICHD) classifies TTH into episodic and chronic. Episodic TTH is defined by fewer than 15 headaches per month and if the headaches occur more frequently and last for longer than 4 hours, the condition is termed as chronic. The intensity of tension headache may vary throughout the day and it can be sometimes difficult to differentiate from migraine.
According to the Migraine Trust the main causes of TTH are anxiety, emotional stress, poor posture and lack of sleep although much of this is mainly based on anecdotal evidence. Most of the people we see have a combination of these factors, but the common denominator for us is often some form of postural stress and other factors such as osteoarthritis of the neck.
Cervicogenic Headache
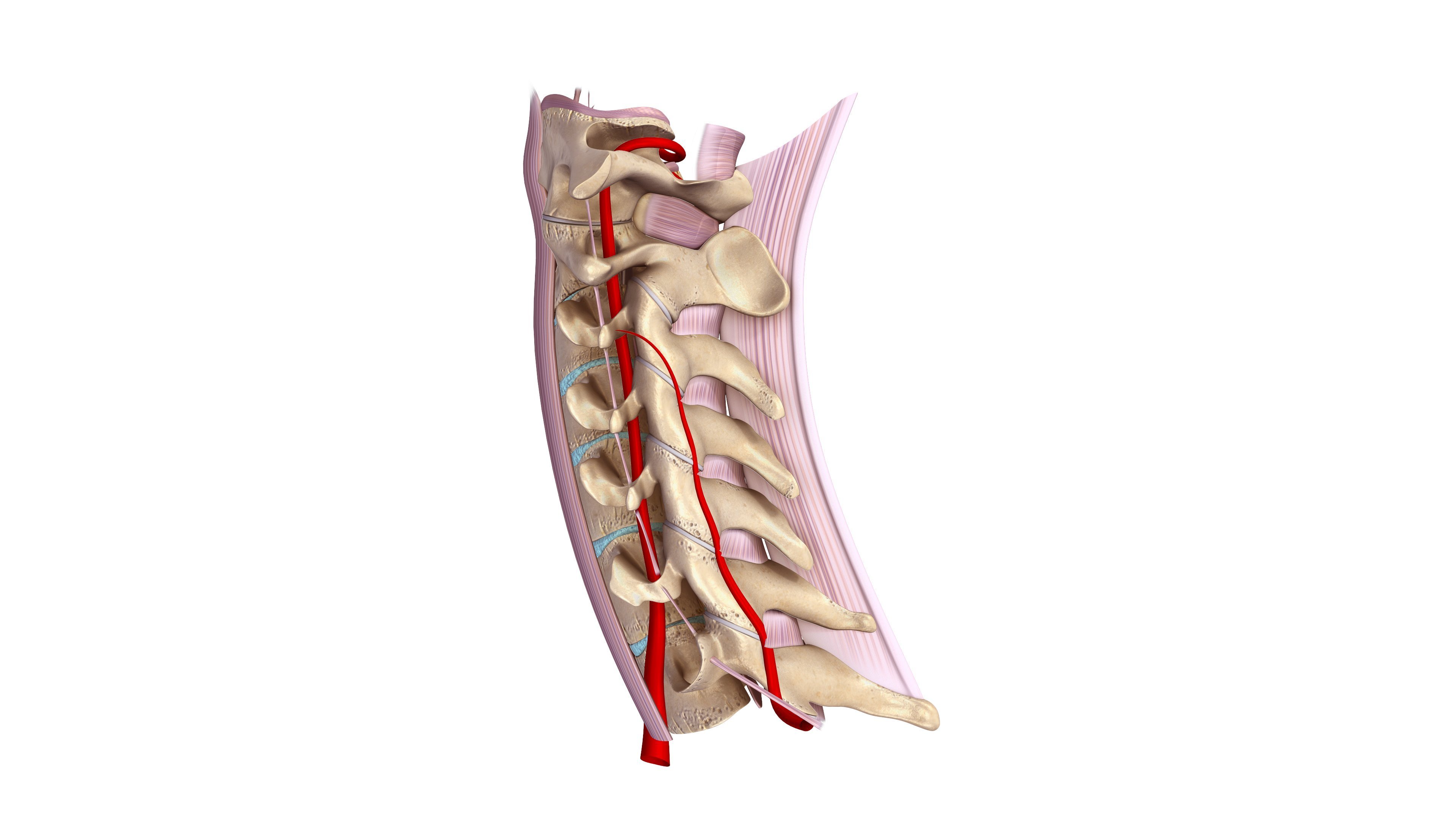
Cervicogenic headaches meanwhile are recognised as a distinct entity in its own right according to the International Association for the Study of Pain. In principle, cervicogenic headache is any headache that originates in either the neck or the back of the head at different segmental levels in anatomical structures; as such it is classed as a secondary headache as it has an indirect causative factor. One or more structures in the neck may be involved, including nerves, the intervertebral disks and the facets joints that join the vertebra together.
For clarity, in the spine, facet joints link the vertebrae at specific segments and are important for preventing excessive rotational and twisting forces which would otherwise damage the intervertebral discs. They also share some of the load bearing of the spine. The correct term for the neck is of course the cervical spine. The cervical spine has seven vertebrae from the first cervical vertebra (or C1) at the top that articulates with the base of the skull through to the seventh (C7) which articulates with our midback or thoracic spine. Most cervicogenic headaches are associated with C2 at the top your neck behind your ear and at C5. C5 is often the level you exacerbate by sleeping in an awkward position or when you accidentally click your own neck due to a sudden unexpected reflexive movement; C5 is also known as the whiplash vertebra for good reason. The pain of cervicogenic headache is usually unilateral; it originates in the neck and then spreads to the frontal and/or temporal areas. The headache initially presents as intermittent episodes and then progresses to an almost continuous pain. Pain may be triggered or exacerbated by neck movement or a particular neck position.
Headaches and Postural Stress
A common denominator in the aetiology of TTH and cervicogenic headaches is sometimes postural stress which is often generated from our workplaces – although our genetics, physiological age and emotional states also factor in. In the modern workplace environment, we can expose ourselves to long periods of postural strain that impose heavy loads on arms, shoulders and neck. This can either be comprised of spending long hours on a computer or behind the wheel of a car.
Although we may be initially unaware of the effects this will eventually lead to an increase in soft tissue tension in the neck and shoulders especially. Eventually you can experience mild discomfort that will quite often improve once you have finished work. This is often the first stage which can last for several weeks or longer. If nothing is done, sometimes the symptoms of RSI can exacerbate, intensify and last longer as they perpetuate. Without treatment, the symptoms of RSI can become constant. We, as osteopaths, can help suggest simple modifications to your workplace. Gentle massage to the tight muscles and manipulation to loosen the joints of the neck, thorax and back can relieve the build-up of muscular tension that may over time lead to headaches.