Cholesterol and Vascular Disease
Posted by Phil Heler, MD on September 6, 2019Too much cholesterol can block your blood vessels. It makes you more likely to have heart problems or a stroke.
Cholesterol is a key factor in heart disease. September is vascular disease awareness month and I will be writing four articles over the forthcoming weeks related to this topic. Vascular disease has an alarming incidence rate. Among adults in industrialised countries, one-fourth of all deaths result from arterial blockages caused by a build-up of plaque (Heron 2013). It has taken a century of research to establish that much of this plaque material is generated by one main causative agent known as low-density lipoprotein (or LDL). LDL is the main transport mechanism for cholesterol. In fact, approximately two thirds of circulating cholesterol resides in LDL. Quite simply if there is too much circulating LDL, and therefore cholesterol, in your blood, it combines with other substances to form plaque which sticks to the walls of your arteries. Plaque formation leads to an increased possibility of various negative clinical outcomes including (but not limited to) coronary and vascular artery disease. Other possible outcome are aortic aneurysms and strokes.

What are lipoproteins?
Cholesterol and other lipids are transported around our body by lipoproteins as a basic building block for cells. Cholesterol and other fats do not dissolve well in blood so they need to be incorporated inside lipoprotein molecules. This helps overcome this problem of solubility because the lipoprotein, as its name suggests, has a protein coated outer membrane (which is readily soluble). This allows lipoprotein molecules to move around the body through the blood and be transported to cells that need them. Basically, lipoproteins are classified into different groups called high density lipoproteins (HDL) or low density (LDL) and very low density (VLDL). Different types of lipoproteins have different purposes.
HDL is seen as beneficial because it carries cholesterol from other parts of your body back to your liver. Your liver then removes the cholesterol from your body. Conversely the job of LDL is to carry cholesterol to target body tissues. However, LDL is seen as detrimental because a high LDL level has a clear correlation with the build-up of plaque in your arteries. VLDL is also regarded as detrimental because it too also contributes to plaque development. But VLDL and LDL have a key difference; VLDL mainly carries other lipids, while LDL mainly carries cholesterol.
Our lipoprotein profiles can change depending on our lifestyles. As many of us know lack of physical activity leads to a lowering of HDL (remember this is the beneficial lipoprotein). Smoking also has the same effect especially in women. Clearly unhealthy eating habits will raise your LDL. US population studies suggest that optimal total cholesterol levels are about 150 mg/dL (3.8 mmol/L). The NHS meanwhile as a general guide recommends that total cholesterol levels should be 5mmol/L or less for healthy adults, and 4mmol/L or less for those at high risk of heart and circulatory diseases.
How does atherosclerotic plaque form?
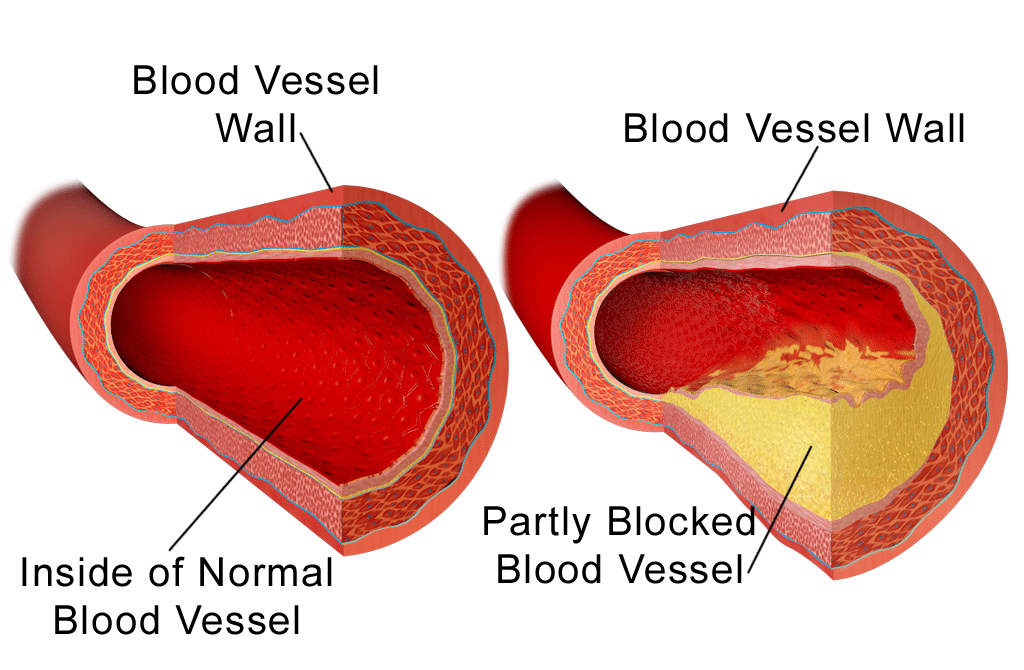
The process through which atherosclerotic plaques develop begins with damage to cells that line the interior surface of blood vessels called endothelial cells. Endothelial cell damage leads to a dysfunction of the blood vessel lining, and this allows LDL particles to permeate through the blood vessel wall. Lipoproteins, especially LDL, can then accumulate within the vessel wall trapped by a cellular matrix in the arterial wall. As more deposits accumulate within the wall of the vessel, smooth muscle cells begin to migrate into the lesion. Ultimately, these smooth muscle cells encapsulate the newly formed plaque forming what becomes ‘fibrous plaque’. Atherosclerotic plaques can lead to partial occlusion of blood vessels and arteries causing decreased blood flow on the other side of lesions and subsequent ischemia (ischemia means a shortage of oxygen for cellular metabolism). Plaques can also rupture, inducing the formation of a thrombus (or blood clot) which can completely block the flow of blood (as occurs in heart attacks or angina).
The Evidence is Robust
There is no denying the sheer weight of evidence that cholesterol is a key driver in the processes of vascular disease even though there is currently a minority of scientific opinion that suggests otherwise. This reminds me of the long-standing joke about the patient who went to see his GP. The GP says “I have good news for you. Your cholesterol has stayed the same. But the bad news is, the research findings have changed!”. However, while guidelines are constantly revised for many health-related subjects (such as alcohol consumption) the recommendations for cholesterol levels have never wavered. Supporting evidence identifying cholesterol as a protagonist in vascular disease has been unequivocal and consistent for decades. Prof Louis Levy, the head of nutrition science at Public Health England (PHE) comments; “There is good evidence that a high intake of saturated fat increases your risk of heart disease. We need to think about where the sources of saturated fat are and how we can reduce them. The largest contributions are dairy products.” The advice from PHE, the World Health Organization, the British Heart Foundation (BHF), Heart UK, other respected institutions and top academics has been very consistent over time. Dairy fats and other sources of saturated fats from lamb, beef and pork (and lots of other seriously tasty foods such as chocolate, baked goods, and deep-fried and processed food) may be fine in modest amounts in a balanced diet, but the saturated fat that they contain is potentially risky.

Cholesterol Levels Worldwide
On a global basis the prevalence of raised total cholesterol increases noticeably according to the income level of the country; a classic example of a ‘disease of affluence’. In low income countries around a quarter of adults have raised total cholesterol, in lower middle-income countries this rises to around a third of the population for both sexes. In high-income countries, over 50% of adults have raised total cholesterol; more than double the level of the low-income countries. More overtly the prevalence of elevated cholesterol is highest in the Region of Europe (54% for both sexes), followed by the WHO Region of the Americas (48% for both sexes). The same figure for African and South East Asian is much lower (22.6% for Africa and 29.0% for Asia).
Some of the statistics regarding cholesterol are mind-bending! Overall, according to the WHO, raised cholesterol is estimated to cause 2.6 million deaths globally (4.5% of total) and 29.7 million disability adjusted life years (or DALYS), or 2.0% of total DALYS. DALYS is yet another horrible acronym but it is quite simple. It is a way of describing the sum of years of potential life lost due to premature mortality and the years of productive life lost due to disability. This is why statins especially have now become widely prescribed.
Cholesterol and Statins
In 2015 The National Institute for Health and Care Excellence (or NICE) recommended that many more of us in the UK should be offered statins. NICE stated anybody who has a 10% chance of a heart attack in the next 10 years – judged on factors including weight, age and blood pressure – should consider taking a statin. It recommended that anyone who had already had a heart attack or stroke should also be strongly advised to take statins. Research suggest that their use is valid. Prof Rory Collins and Professor Richard Peto are two leading epidemiologists at Oxford University of Oxford who have been amassing a huge database on statins since 1994. So, when it comes to statins, there is a huge database of research at their disposal. They have published many papers. In 2016, in a major review in the Lancet, they concluded that lowering cholesterol over five years with a cheap daily statin would prevent 1,000 heart attacks, strokes and coronary artery bypasses among 10,000 people who had already had one. The figures suggest that their use would also prevent 500 such incidents in people who were at increased risk, due to high blood pressure or diabetes. Prof Rory Collins commented at the time; “Our review shows that the numbers of people who avoid heart attacks and strokes by taking statin therapy are very much larger than the numbers who have side-effects with it. Most side-effects can be reversed by stopping the statin – but heart attacks cause permanent damage. Consequently, there is a serious cost to public health from making misleading claims about high side-effect rates that inappropriately dissuade people from taking statin therapy despite the proven benefits.”
While raised total cholesterol is no doubt a major cause of disease in both the developed and developing world, even small changes in your diet can make a huge difference. Research suggests that even only a 10% reduction in serum cholesterol in men aged 40 leads to a 50% reduction in heart disease within 5 years. In Ireland, there has been an impressive 30% reduction in the heart disease death rate. This impressive reduction has been attributed to only 4.6% reduction in cholesterol. In the meantime, it is important to point out that cholesterol does actually have a really important role in your body. We require it to make hormones, vitamin D, and substances that help you digest foods. Cholesterol is used to help the liver create bile which aids us in digesting the food that we eat. Without bile our bodies are unable to properly digest foods, especially fats. Cholesterol is also a structural component of cells and along with other fats (or lipids) it helps make up the structure of each and every cell in our bodies. Cholesterol is there to basically provide a protective barrier.